
Getting Back To It
personal update and miscellany


It’s been a while since I’ve written anything lately, and that doesn’t feel good. My writing voice has always been loadbearing to my identity, and if I don’t have anything to say, if I’m not “appearing in public”, it’s a little bit destabilizing. Invisibility can be comfortable (and I’m less and less at home with the aggressive side of online discourse these days) but it’s also a little bit of a cop-out.
The fact is, I’ve been hiding. It feels like “writer’s block” or like I “can’t think of anything to say”, but obviously that’s suspect, and the real thing is that I can’t think of anything to say that’s impeccable and beyond reproach and definitely won’t get criticized. Also, it’s clearly a vicious cycle; the less I participate in public life, the fewer discussions I’m part of, and the fewer opportunities I have to riff off of what other people are saying.
Life Stuff
So what have I been up to?
Well, for one thing, I had a baby.
For another, I’ve been job hunting.
Solo consulting was fun, but I wasn’t getting many clients, and I’m eager to get back to working on a team again.
What kind of am I looking for? Mostly AI-related stuff, on the research or applications side. Bonus points if there’s an AI-for-science connection.
Stuff I have experience doing and would be interested in doing again:
running analytical, statistical, or ML experiments
building “wrapper” tools around LLMs
working with coding agents
lit review and due diligence, particularly in life sciences
financial analysis, market research, and associated business strategy
Stuff I’m frequently told I’m good at:
learning fast
taking initiative
writing
being honest and operating in good faith
I’m looking at some opportunities at the moment, but I’m also interested to hear about new things, if you know of anything that might be a good fit.
Projects
Messing around with Claude Code continues to be fun; a lot of what I’ve been doing lately has been tools for personal use.
I have my little life-tracker app:




which is an all-in-one diary, to-do list, mood tracker, and place to keep track of other things I log (books I read, dishes I cook, notes from meetings with people, etc). It’s largely replaced my Roam and and Complice to-do app.
I also made a personal CRM from my email contacts:
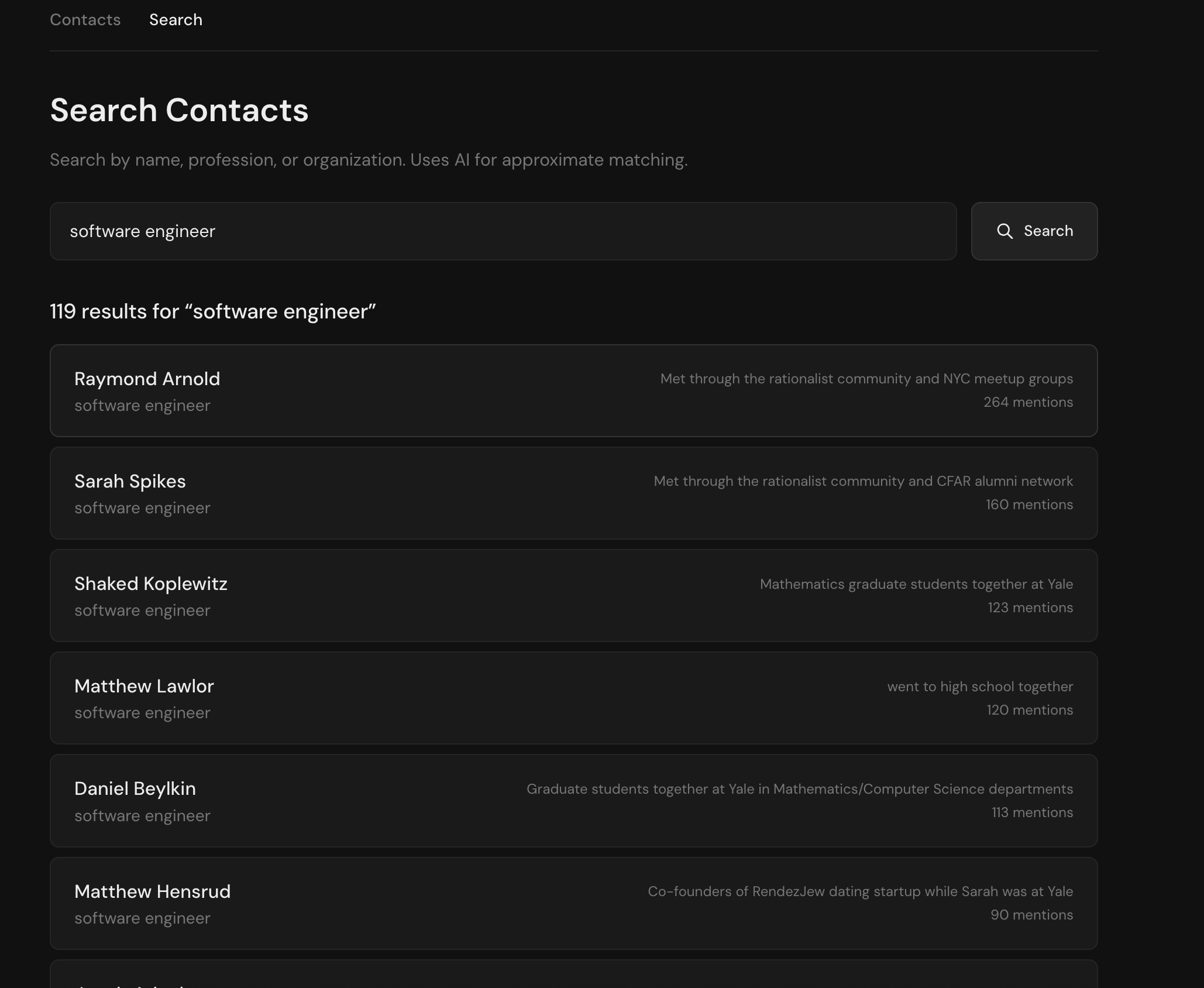
and used Claude analysis of email text and web search to identify all contacts by how we know each other, their current profession and employer, and their current location.
So now I can search for things like “who do I know who’s a software engineer” or “who do I know in NYC”.
The personal CRM project has actually been really helpful for getting me off my butt to reach out to more people to meet in person for lunch or coffee.
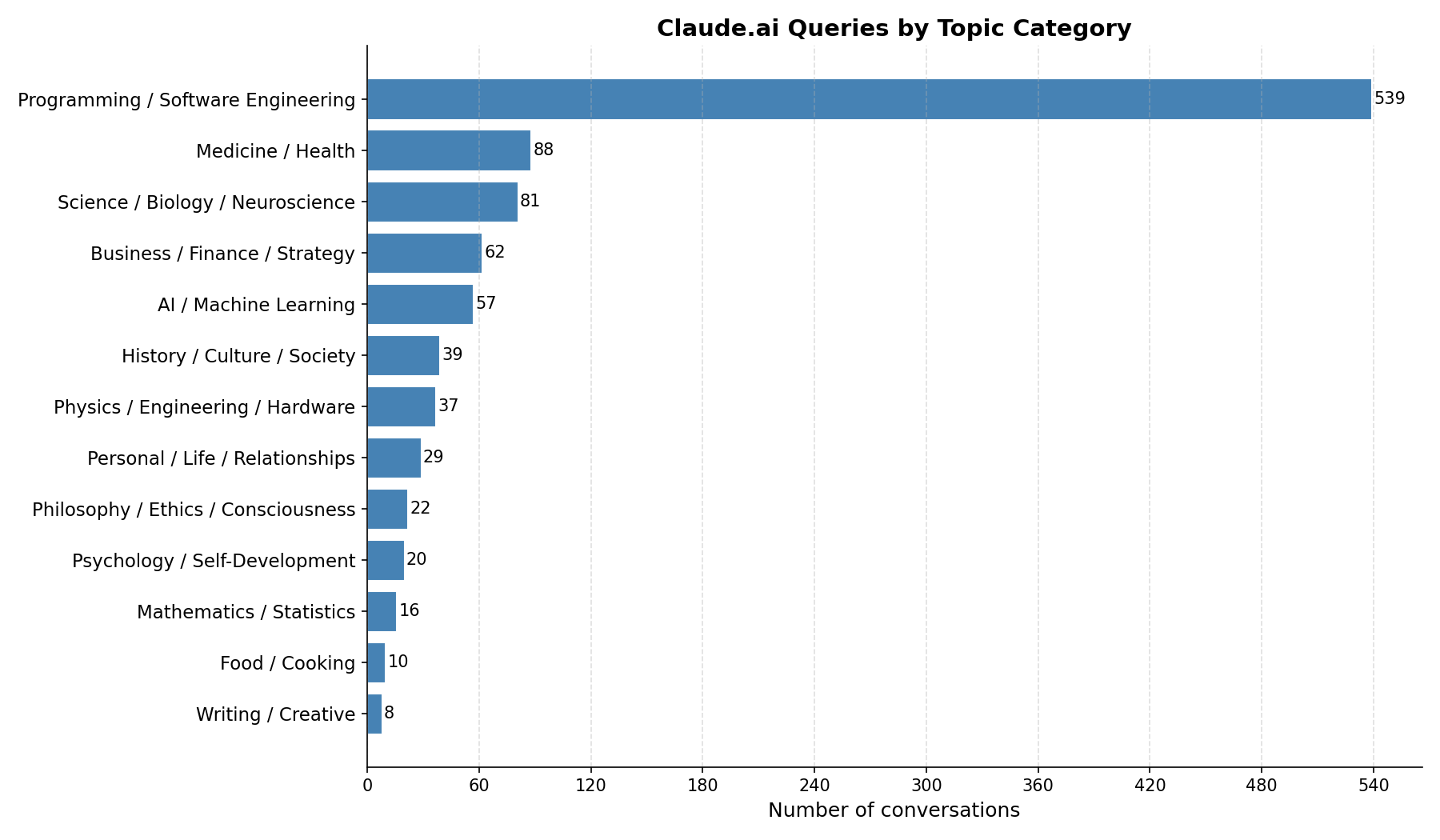
Other stuff includes analyzing my Claude use:
and my personal finances (not as helpful as some people have found; I did find some unnecessary expenses I could cut, but overall it turns out I don’t do much overspending).
25 Miscellaneous Opinions
Some things that are top of mind, not necessarily brilliant or original, just as a way of priming the pump about sharing my point of view.
I’m mostly not doing high-level AI predictions any more; it’s hard enough to keep up with the present without trying to foretell the future.
I’m an enthusiastic AI user but I’m more sympathetic than you’d guess to hardcore anti-AI people. IMO every proposed use case for AI should have a grognard insisting that it’s terrible and going to ruin everything, and that will force enthusiasts to think harder about where it adds value and where it just adds error, degrades quality, or enables bad behavior at scale.
I hate AI-assisted writing and am increasingly disillusioned with AI art; I do value the human touch, both for social reasons (I want to hear from someone in particular; part of what I value in a piece of writing is the fact that I now know what John Doe’s opinion is) and for reasons of diversity/originality.
The DOD ordering Anthropic to remove safeguards is indeed terrible.
I think Claude has better ethics than the average person on Earth.
I don’t buy the Citrini post. When has any technology caused a recession by being too good? Job loss, yes. Inequality, yes. Social upheaval, even to the point of war, yes. But an aggregate demand shock, where the tech makes goods so much cheaper that it causes a financial crisis? Without people buying more of something else with their newfound spare cash? I don’t know that this has ever happened.
I do see a possibility that custom software (made by you + coding agents) becomes a new competitor to mass-produced software sold by SaaS companies. I’m not sure how much this kills SaaS, though, or if they even find a way to turn this to their advantage (cutting their own costs? adding more customizability now that it’s so cheap?)
I think closed-loop “AI scientists” where the AI proposes experiments, implements them automatically, analyzes the data, and does it all over again, are probably not already happening at scale today. They are doing R&D and early experiments in startups, and I expect we’ll see unambiguously “closed loop” processes announced, at least at demo scale, this year or next; my impression is that startups are farther ahead on this than big pharma, which seems to still be hiring the first members of their in-house teams for this sort of thing. I continue to think fully automated, closed-loop experimentation makes more sense for biological HTS than anything else, including materials.
I think eventually we’re going to saturate artificial benchmarks and for continued AI progress we’ll need some kind of real-world ground truth that makes “superhuman performance” even meaningful. In math and code that can mean RL against proof assistant and compiler feedback, for instance. In forecasting it might mean RL against true outcomes. In natural science it ultimately might mean problem-solving/troubleshooting/world-modeling a real physical environment.
I’m genuinely uncertain whether I’m more in the “harness” or “model” camp, in terms of what’s more important; for some things, the right “harness” (system prompts, product scaffolding, hard-coded details) makes a less powerful model more useful than a more powerful model “out of the box”, but for other things, the “out of the box” default choices are actually great and the “harness” is irrelevant. (And there’s a third case where the “harness” is basically “a way to turn way more tokens into way better results”, which is sometimes worth it, sometimes not.)
I think universalism has a particularism all its own. For example, “cosmopolitanism” as opposed to nativism, being favorably disposed towards foreigners, is often informed by specific life experiences (in my case, living in a port city; being raised in the highly international culture that is academia; being descended from millennia of traders and travelers). It’s not abstract or bloodless; it is grounded in very specific, concrete places and people, and I like those places and people! It is fine to have ingroup loyalty; why should our ingroup be any different, just because we’re also objectively correct?
I think it’s impossible to both be “confident” and never be annoying to anyone. Strong, bold people usually get on someone’s nerves.
I think a root cause of the problems with healthcare in developed countries might be that we’re pathologically unwilling to admit to healthcare scarcity. It takes a long time and a lot of bureaucratic hoop-jumping to find out that a particular form of healthcare is not available to you, as a patient.
In my grandfather’s day, when he was a country doctor, poor uninsured patients often had to go without healthcare that they couldn’t afford. Today, thankfully, more people can afford more healthcare…but it is much less straightforward to find out what you can’t afford, or can’t access at any price, and that means nobody can do any planning around the scarcity that does, in fact, still exist.
“Healthcare abundance”, as an agenda of building more hospitals, licensing more healthcare practitioners, producing more drugs and supplies so we’re not in shortage all the time, etc, is very important, but it is harder to communicate than housing abundance, in part because most people don’t know healthcare scarcity is a thing. And people don’t know about healthcare scarcity because we hide it.
We’re also really weird about death. That’s mostly a problem with the general public, though medical professionals sometimes contribute to it. People are really way less frank than they should be about situations like “Grandpa will never get well”, “you are dying and additional treatment will extend life weeks, not months”, “you probably want to die at home not in the hospital”, “here are some tips and tricks for having a good hospital stay if you’re ever severely ill, because statistically speaking one day you will be”, etc. People don’t want to think about the bad outcome! And doctors aren’t necessarily straightforward about telling you the bad outcome!
I think analytical, “optimizer”, spreadsheety people get a lot of hate that’s undeserved. You do, in fact, want to get the facts right, pursue goals, and simplify away what’s extraneous. A lot of processes get better when someone more “spreadsheet-brained” comes in and reforms them.
Since I’ve had kids, I’ve become more pro-video game, more anti-TV (including and especially YouTube), and more pro-incentives (rewards more so than punishments, but both are fine IMO when reasonably implemented).
I think “preparing your kids for an uncertain future” primarily means getting them good at fully general skills — reading, writing, and arithmetic, plus social skills and physical fitness — and being flexible about the rest, and building a good enough relationship with them that they might ever listen to you as young adults. Also, it turns out that most parents and schools don’t really care how good kids are at the “3 R’s”, and if you care, you have to treat it like a niche preference and get creative about making sure it happens.
I think freedom is good, for kids and adults. All else equal, if somebody wants to do a thing, and there’s not a good reason to stop them, they should be allowed to do as they please. There are all sorts of exceptions and edge cases, but “things are allowed by default, forbidden only for good reasons” is a core principle for me (and one that disappointingly few people share!)
There’s some concept of “wholesomeness” that has become a bigger part of my life as I’ve gotten older. Some combination of “do things you’re comfortable being transparent about to a general audience, including children and people significantly older than you”, “do things that don’t cause a lot of negative consequences”, “stay on the ‘light’ side more than the ‘dark’ side aesthetically and tonally”, “avoid actions motivated by hostility”, etc.
I really prefer history and social science books written in the 19th or early 20th century. There’s a point where it started to be taboo to editorialize too much, to describe personalities or give authorial opinions; but an opinionated guy telling stories about individuals is a much more entertaining and clear way to learn an otherwise dry subject than interminable abstraction.
To the extent I have been developing software “taste” it’s really just caution. Use common languages and frameworks. Try not to build anything elaborate if you can avoid it. Write comments. In principle (though I have less experience with this myself) it seems obviously better to use systems that make it harder to produce bugs (e.g. type-checking.) Remember, Thou Art Mortal.
For the most part I have uncreative tastes — I like prestige TV, fancy restaurants, swanky-but-mainstream graphic design. Books and music are the only place where I’m actually far away from “generic coastal elite” taste.
I think more people should donate to stuff based on personal taste, “seems cool to me”, “I know the guy and he’s neat”, those kinds of casual considerations. There’s no shame in it! You don’t have to only donate when there’s an impeccable Process in place! You can donate small amounts (relative to your income/wealth), that you can comfortably afford, as almost a consumption good. Buying stuff you want to see more of in the world.
Macrophages are my favorite immune cell and I have a good feeling about any tactic that works with em. The innate immune system in general is underrated.
Simplicity, generally, is underrated as a heuristic in biology — “we should work with this biological system because we have any hope of understanding it.” Evolutionarily ancient things (the innate immune system, the hypothalamus) are going to be more tractable to study in animals, and simpler overall.
I missed you! Welcome back to the land of the public-facing! That was going to be all, but instead:
13. This was surreal commentary to me, because I used to work in health insurance where EVERYONE knows healthcare is scarce, and instead has ideological or pragmatic disagreements about which parts SHOULD be scarce (million dollar gene therapy? drugs that are technically approved but don't really work? convenience drugs that don't technically work better than taking the two meds separately except that they improve adherence by improving convenience? how much do you need to improve adherence before it's worth it?) or how to make parts that are supply-side scarce (rather than unaffordable on the demand side) like rural specialist access less scarce (okay, actually there's an aside to be had there about insurance networks that make all the "preferred" providers with preferential pricing be providers who are in urban areas, so if you have members of the plan who live rurally, well, too bad for them).
There is, yes, also the issue of the inability to discover whether a treatment for your condition exists at any price (I like IncitefulMed as a first pass search, but that's not a solution, just a search engine better than most; OpenEvidence will do too, and is still not a solution, just a tool), and the separate issue of trying to determine what the treatment costs, which there is an entire industry of band-aid solutions for that DO NOT SOLVE THE PROBLEM, which really just tells you how Byzantine the problem is. But I'm skeptical of the idea that unwillingness to admit to scarcity is a root cause of problems with healthcare policy in the US, just because policymakers and insurers explicitly argue about what should be scarce in healthcare and entirely the patient's responsibility to pay for, all the time.
(I'm less sure about other developed countries, but Singapore presents scarcity of total $$ relative to the rising cost of the package of care the government thinks of as normal AS the problem--or rather, American studies of Singaporean healthcare suggest that Singaporean policymakers believe so; take with the usual grains of salt.)
You can claim that the general public refuses to acknowledge scarcity and thinks everything should be paid for, maybe, (I'm not talking about socialized medicine as a concept; I'm talking about what's on the formulary/billing code book of reimbursed medicine, socialized or commercial) but I'm not convinced that has any impact on policy, especially compared to a lobby group like say the AMA, AHIP, or PhRMA.
20. You're probably already reading it because of the social circle you're in, but I strongly recommend Ada Palmer's Inventing the Renaissance if you like history books that are an opinionated girl telling entertaining stories about interesting individuals, and of course, the Italian Renaissance.
11. "why should our ingroup be any different, just because we’re also objectively correct?" - I literally laughed out loud, and since you could not see this, I felt I should interact socially by telling you so. I too am from a port city and grew up in the highly international culture that is natural sciences academia. You would think that hearing so many people speak English as a second language and being delighted to hear about where they came from would make me less afraid to interact in languages that I only kind of speak, but alas, it does not.
PS: Your baby is cute!
Really glad you published this. The premise and the form is inspiring. Makes me wanna shake off the rust and write again, too. Also, Bruce is a boss name.