


All The Latest Human tFUS Studies
What's new in ultrasound neuromodulation?

Transcranial focused ultrasound neuromodulation — altering the brain’s activity with low-intensity ultrasound — is really exciting .
It allows us to manipulate arbitrary regions of the brain without surgery, potentially replacing the (brain-damaging) electrode implants currently used for serious neurological conditions like epilepsy and Parkinson’s, and potentially also expanding applications of brain stimulation to milder conditions not worth the risks of brain surgery, like mental illness, addiction, or chronic pain.
The field is rapidly growing, and since I wrote my earlier post series there have been quite a few human studies published. Here’s a systematic overview of all the human studies published in 2024, by target brain region.
Headline Results
This year’s papers further confirm, to start with, that ultrasound does things to brain activity, if that was still in doubt, and that it is safe enough to run human experiments with (no adverse effects during experiments with small numbers of participants and brief exposures.)
There are notably inconsistent results in whether targeting ultrasound to a given brain area increases or decreases neural activity in that area, even in some cases when the same area is targeted with the same sonication parameters! We clearly need to get a better sense of what ultrasound even does.
Most studies don’t do the obvious (but admittedly expensive) thing of confirming a change in neural activity via a noninvasive measure like fMRI. Those that do, show different results (more activity in the targeted region, less activity in the targeted region, or neither) depending on which region is targeted; this tells us that “tFUS” as a class doesn’t have a globally consistent effect on targeted neural activity. Again, still more to learn.
However, despite the primitive state of our understanding of this modality, we do already seem to have some strikingly useful results. Ultrasound stimulation of the thalamus seems to be helpful for essential tremor, stimulation of the posterior insula seems to reduce pain sensitivity, and stimulation of the anterior medial prefrontal cortex seems to have quite strong effects on depression. These are before vs. after results without a control group, not randomized controlled studies, but I think they at least warrant followup.
I’m not as excited as I’d want to be about Jay Sanguinetti’s default-mode-network-inhibition study. The effects seem subtle and game-able; and anecdotally the stories I hear from people who’ve tried the protocol from his lab are not “I was in a clearly altered state”.
But all in all, it continues to be a promising field; tFUS clearly does things, some of those things may be useful, and the more data we get, the closer we’ll get to an actual model of what it does.
Amygdala
Chou, et al1 at Harvard Medical School tested tFUS2 on the left amygdalas of 30 healthy volunteers. Compared to sham stimulation, tFUS resulted in less fMRI-measured activity in the amygdala.
The amygdala is involved in fear responses, so reducing amygdala activity could have uses in anxiety disorders and phobias.
Hoang-Dang, et al3 at UCLA used tFUS4 on the right amygdala of 21 older adults, and found no effect on state anxiety after tFUS, but did show an increase in negative emotional reaction to viewing negative images. There was also a significant increase in heart rate between trials of this mildly stressful task.
Since the amygdala is usually active during fear, this suggests that these stimulation parameters may have activated the amygdala…despite the other study using similar parameters and showing a direct decrease in amygdala activity. The UCLA study doesn’t mention the duration of tFUS stimulation, which may be a relevant factor.
Ideally, to resolve this confusion, we’d need to see a study that measures both amygdala activity and behavioral/physiological measures of anxiety, and specifies all the sonication parameters including duration.
Motor Cortex
Zeng, et al5 at the Krembil Research Institute in Toronto applied theta burst transcranial ultrasound6 on 14 healthy subjects, and found that the motor evoked potential from concurrent rTMS stimulation was higher with higher-intensity ultrasound stimulation (20 W/cm^2 vs 10), medium PRF (5 Hz vs 2 Hz or 10 Hz), higher duty cycle (10% or 15% vs 5%), and longer sonication (120s vs 80s or 40s). This indicates that ultrasound stimulation can make the human motor cortex more “excitable” in response to a given stimulus. However, ultrasound did not decrease the resting motor threshold, i.e. it didn’t make the motor cortex more sensitive to a smaller electic stimulus.
Zadeh, et al7 at the University of Calgary tested tFUS to the primary motor cortex on 21 healthy individuals, with various stimulation parameters8; a significant decrease in motor evoked potential was seen in the 10 Hz and 100 Hz pulse repetition frequency stimulation conditions, with the biggest decrease in the 100 Hz pulse repetition frequency.
Clearly we still have a lot to learn about what happens to the motor cortex under tFUS stimulation; the two studies are consistent with a story of “high PRF is inhibitory, low PRF is excitatory” but until a single experiment compares the whole range of sonication parameters we can’t be sure.
Nucleus Accumbens
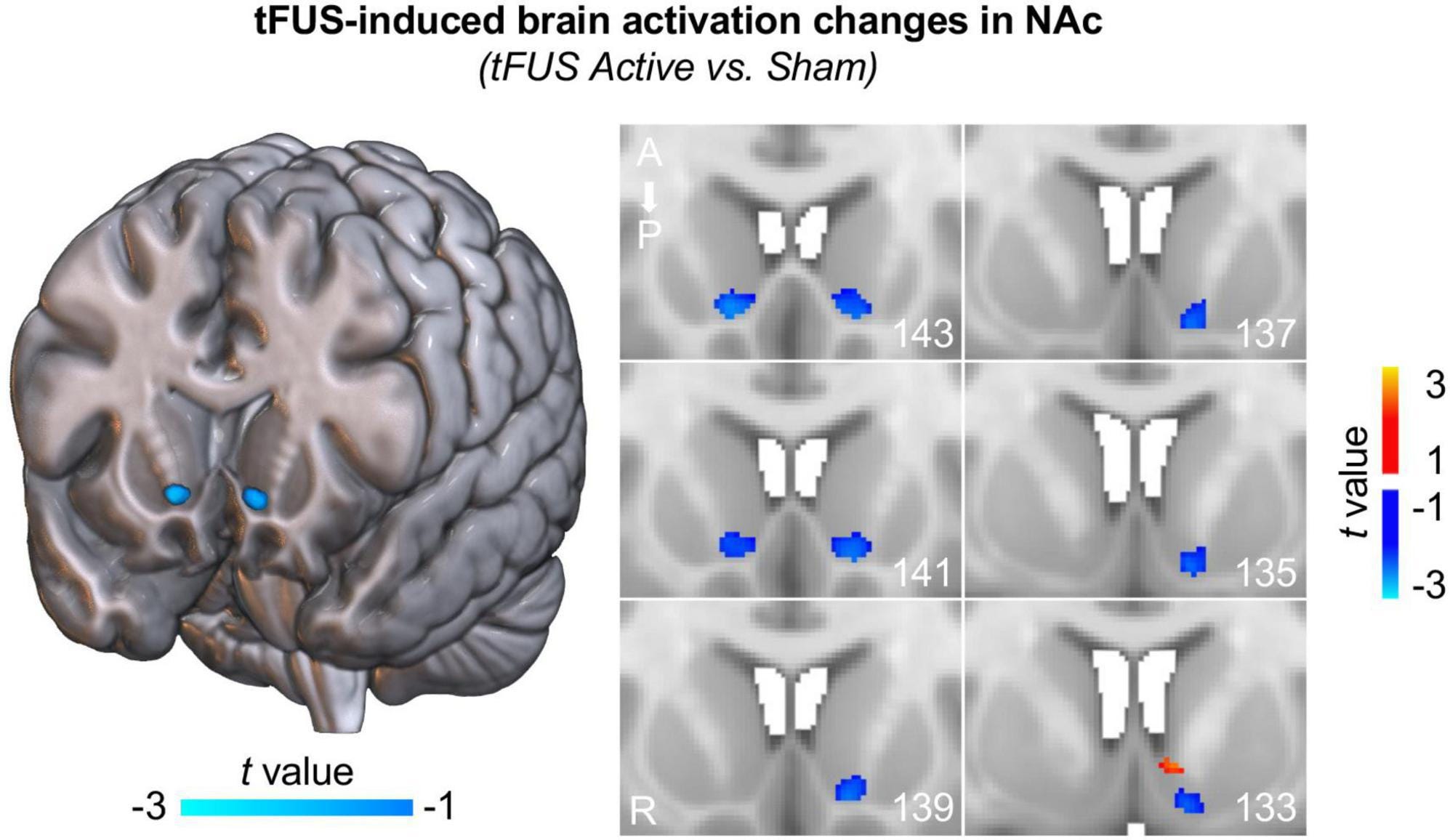
Peng, et al9 at the Medical University of South Carolina tested tFUS on the left NAc in 10 healthy volunteers, for ten minutes.10 Compared to sham stimulation, tFUS inhibited activity (as measured by fMRI) in the bilateral nucleus accumbens.
The nucleus accumbens is active during perception of both rewards and threats, so inhibiting it may have uses for addictions or phobias.
Posterior Cingulate Cortex
Lord et al11 at the University of Arizona applied tFUS12 to the posterior cingulate cortex of 30 healthy subjects, and found an increase in score on the Toronto Mindfulness Scale (compared to sham stimulation), and a decrease in functional connectivity in the default mode network. There was no significant effect on mood, but a significant decrease in “global vigor”, and an increased rate of reporting a distorted sense of time, loss of ego, and seeing events from one’s past.
“Functional connectivity” means the correlation between the activity of brain regions as measured by fMRI; two regions are functionally connected if they are active/inactive at the same times.
The default mode network is a system of brain regions, including the posterior cingulate cortex, which are generally functionally connected in humans and other mammals; it is most active when someone is not engaged in any particular task but is thinking about oneself or one’s autobiographical memories.
One theory of the mechanism of mindfulness meditation is that it turns down the activity of the default mode network, and thus the “sense of self” derived from thinking about yourself. This experiment seems designed to suggest that tFUS can have a meditation-like effect.
Posterior Insula
In et al13, at Virginia Tech, treated 16 volunteers with low intensity focused ultrasound14 to the posterior insula reduced subjective pain rating from repeated exposure to a heat stimulus. The higher the pressure applied to the brain, the lower the pain rating. Other regions of the brain had no effect.
Prefrontal Cortex
Schachtner at al15, at the University of Arizona, treated twenty patients with depression with up to 11 sessions of transcranial focused ultrasound16 to the anterior medial prefrontal cortex. 35% met remission criteria from depression; mean BDI depression score decreased from 39 to 28 (p <0.001).
Thalamus
Bancel et al17, at PSL University in Paris, tested tFUS18 targeted to the ventral intermediate nucleus of the thalamus in 9 patients with essential tremor. 5/9 patients were “responders” who saw a reduction in tremor, sustained after the neuromodulation ended.
Martin et al19, at University College London, tested tFUS20 targeted at the lateral geniculate nucleus of the thalamus on seven healthy participants. During a visual task, tFUS stimulation of the LGN led to higher fMRI-measured activity in the LGN (compared to sham stimulation) and also to higher activity in a region of the ipsilateral visual cortex.21 Also, 40 minutes after stimulation, that same region of the ipsilateral visual cortex is less active during visual tasks.
Deveney et al22, at UCLA, treated 10 patients with essential tremor with eight 10-minute ultrasound sessions23 targeted to the ventral intermediate nucleus of the thalamus. All 10 patients saw decreases in tremor scores, significant at p < 0.001; patients were more able to draw regular spirals (a standard test of hand tremor.)
Riis et al, at the University of Utah, treated 3 patients with essential tremor with tFUS24 targeted to the ventral intermediate nucleus of the thalamus. 2/3 patients saw almost complete cessation of tremor; one patient had no significant effect.
Ventral Capsule/Striatum
Chou at al25 at Harvard Medical School tested tFUS26 targeted at the ventral capsule/ventral striatum in twelve healthy individuals, and found increased activation in the putamen during a reward task with the 10Hz PRF setting, but not with the 125 Hz PRF setting.
Visual Cortex
Kossnoff, et al27 at Carnegie Mellon tested 25 healthy human subjects with a combination of tFUS28 to the V5 region of the visual cortex, and a noninvasive brain-computer interface designed to enable the user to spell words with their mind. Adding tFUS reduced mean error (13.3% vs 15.5%) and median error (0.0% vs 11.8%) in spelling.
Chou, Tina, et al. "Transcranial focused ultrasound of the amygdala modulates fear network activation and connectivity." Brain Stimulation 17.2 (2024): 312-320.
20 minutes, 30s on, 30s off; PRF = 10 Hz, PW = 5 ms, DC = 5%, derated ISPPA = 14.4 W/cm2, derated ISPTA = 0.72 W/cm2, fundamental frequency = 0.65 MHz
Hoang-Dang, Bianca, et al. "Transcranial Focused Ultrasound Targeting the Amygdala May Increase Psychophysiological & Subjective Negative Emotional Reactivity in Healthy Older Adults." Biological Psychiatry Global Open Science (2024): 100342.
PRF = 10Hz, PW = 5 ms, DC = 5% , ISPTA = 0.72 W/cm2, fundamental frequency = 0.65 MHz
Zeng, Ke, et al. "Effects of different sonication parameters of theta burst transcranial ultrasound stimulation on human motor cortex." Brain Stimulation 17.2 (2024): 258-268.
acoustic intensity (AI) = 10 and 20 W/cm2; pulse repetition frequency (PRF) = 2, 5, and 10 Hz; duty cycle (DC) = 5%, 10%, and 15%; sonication duration (SD) = 40, 80, and 120 s, fundamental frequency 0.5MHz
Zadeh, Ali K., et al. "The effect of transcranial ultrasound pulse repetition frequency on sustained inhibition in the human primary motor cortex: A double-blind, sham-controlled study." Brain Stimulation 17.2 (2024): 476-484.
PRF = 10 Hz, 100 Hz, or 1000 Hz; DC = 2%; ISPTA = 0.5 W/cm2; ISPPA = 5 W/cm2
Peng, Xiaolong, et al. "Non-invasive suppression of the human nucleus accumbens (NAc) with transcranial focused ultrasound (tFUS) modulates the reward network: a pilot study." Frontiers in Human Neuroscience 18 (2024): 1359396.
30s “on”, 30s “off”, repeated ten times. Fundamental frequency = 650 kHz, Pulse repetition frequency = 10 Hz, Pulse width = 5 ms, Duty cycle = 5%, Sonication duration = 30 s, ISPTA = 719 mW/cm2
Lord, Brian, et al. "Transcranial focused ultrasound to the posterior cingulate cortex modulates default mode network and subjective experience: an fMRI pilot study." Frontiers in Human Neuroscience 18 (2024): 1392199.
acoustic frequency (AF) = 500 kHz, pulse repetition frequency (PRF) = 10.526 Hz, pulse repetition period (PRP) = 95 ms, pulse duration (PD) = 5 ms or 2,500 cycles, duty cycle = 5.26%
In, Alexander, et al. "Low-intensity focused ultrasound to the posterior insula reduces temporal summation of pain." Brain Stimulation (2024).
PRF = 1 kHz, duty cycle = 36%, ISPPA = 4.2 W/cm^2, ISPTA = 1.5 W/cm^2, total time = 600 s, 1 s on and 5 s off
Schachtner, Jessica N., et al. "Transcranial Focused Ultrasound Targeting the Default Mode Network for the Treatment of Depression." medRxiv (2024): 2024-05.
acoustic frequency = 400 kHz, pulse duration = 5 ms, pulse repetition rate (PRR) = 10 Hz, a maximal spatial peak/temporal average acoustic intensity = 670 mW /cm2,, peak negative pressure 820 kPa.
Bancel, Thomas, et al. "Sustained reduction of essential tremor with low-power non-thermal transcranial focused ultrasound stimulations in humans." Brain Stimulation 17.3 (2024): 636-647.
acoustic frequency = 650kHz, PRF = 0.07-167 Hz, duty cycle = 5-33%, Isppa = 19.8 W/cm2
Martin, Eleanor, et al. "Ultrasound system for precise neuromodulation of human deep brain circuits." bioRxiv (2024): 2024-06.
acoustic frequency = 555 Hz, 300 ms pulses every 3 seconds, target pressure of 775 kPa; and 20 ms, 5 Hz, theta burst stimulation for a total of 80 s
ipsilateral = same side. (i.e. stimulating the left LGN results in more activity in the left visual cortex.)
Deveney, C. M., et al. "Transcranial focused ultrasound for the treatment of tremor: A preliminary case series." Brain Stimulation 17.1 (2024): 35-38.
acoustic frequency of 650 kHz, pulse width of 5 ms, duty cycle of 5 %, a pulse repetition frequency of 10 Hz, ISPPA. of 14.39 W/cm2, ISPTA.3 of 719.73 mW/cm^2, Mechanical Index of 0.75 and Peak Negative Pressure of 0.61 MPa
acoustic frequency: 650 kHz, 0.72 MPa peak pressure following correction for the skull) every 100 ms over the 15 s total sonication duration, ISPPA of 1.612 W/cm^2
Chou, Tina, et al. "A Low-Intensity Transcranial Focused Ultrasound Parameter Exploration Study of the Ventral Capsule/Ventral Striatum." Neuromodulation: Technology at the Neural Interface (2024).
PRF = 10 Hz, PW = 5 ms, 5% DC
Kosnoff, Joshua, et al. "Transcranial focused ultrasound to V5 enhances human visual motion brain-computer interface by modulating feature-based attention." Nature Communications 15.1 (2024): 4382.
tFUS at 0.2 MPa peak-peak pressure, 3 kHz pulse repetition frequency, 700 kHz fundamental frequency, pulse duration: 200 µs, sonication duration: 500 ms
Needless to say, and I’m sure you already know this, but I’ll say it anyway because it’s worth emphasizing: “…whether targeting ultrasound to a given brain area increases or decreases neural activity in that area…” is a very narrow slice of the more important question of “…whether targeting ultrasound to a given brain area changes what it’s doing, and if so, what is the nature of that change…”.
Separately, it’s annoying that Martin et al. did a whole project on stimulating LGN without asking volunteers if they noticed anything funny about their vision. Or if they did ask the volunteers that question, then it’s annoying that they didn’t say anything about it in their biorxiv paper. Unless I missed it. One might cynically assume that the volunteers didn’t notice anything unusual, and the researchers left it out of the paper because it would make their experiment seem less exciting.
Speaking of which, anecdotal hearsay datapoint: I have a friend of a friend with access to a tFUS research setup. They stimulated their own nucleus accumbens, and didn’t feel anything. (I don’t know what parameters they used or anything.)
Positive results, negative results, no results, increased blood flow, decreased blood flow, no changes in blood flow. Is it reasonable to postulate that what’s being picked up on fMRI is not changes mediated by ultrasound but instead just changes in an undulating system? Seems likely to me.